What we're working towards
Real-world feedback loops
RL drove the last leap in the domains with a fast, clean reward signal in code and math. In medicine the feedback on whether a decision was right is slow and noisy, and it can only come from real clinical practice.
Robust across the long tail
Medicine has a long tail of rare cases, and the rare one is often what matters most. We train for the tail, where models built on the common case fall apart.
Specialisation without forgetting
Training a model on a domain tends to erode what it already knew. We add deep clinical capability while keeping the model's general reasoning intact.
Long-horizon reliability
Models stay sharp for a few steps and drift over many. A clinical case runs for days and dozens of decisions, which puts us straight onto the frontier's long-horizon problem.
Knowing what it doesn't know
A confidently wrong model is dangerous in a clinic. Calibration, abstention, and sensing the edge of its own competence are open reliability problems a real colleague has to get right.
One model across modalities
Clinical judgment spans pathology, radiology, labs, and genomics. We train a single model to reason across them, on top of modality encoders we have built in house.
Research
The Vortex line
Frontier-scale, multimodal agentic reasoning models for medicine. Our flagship model.
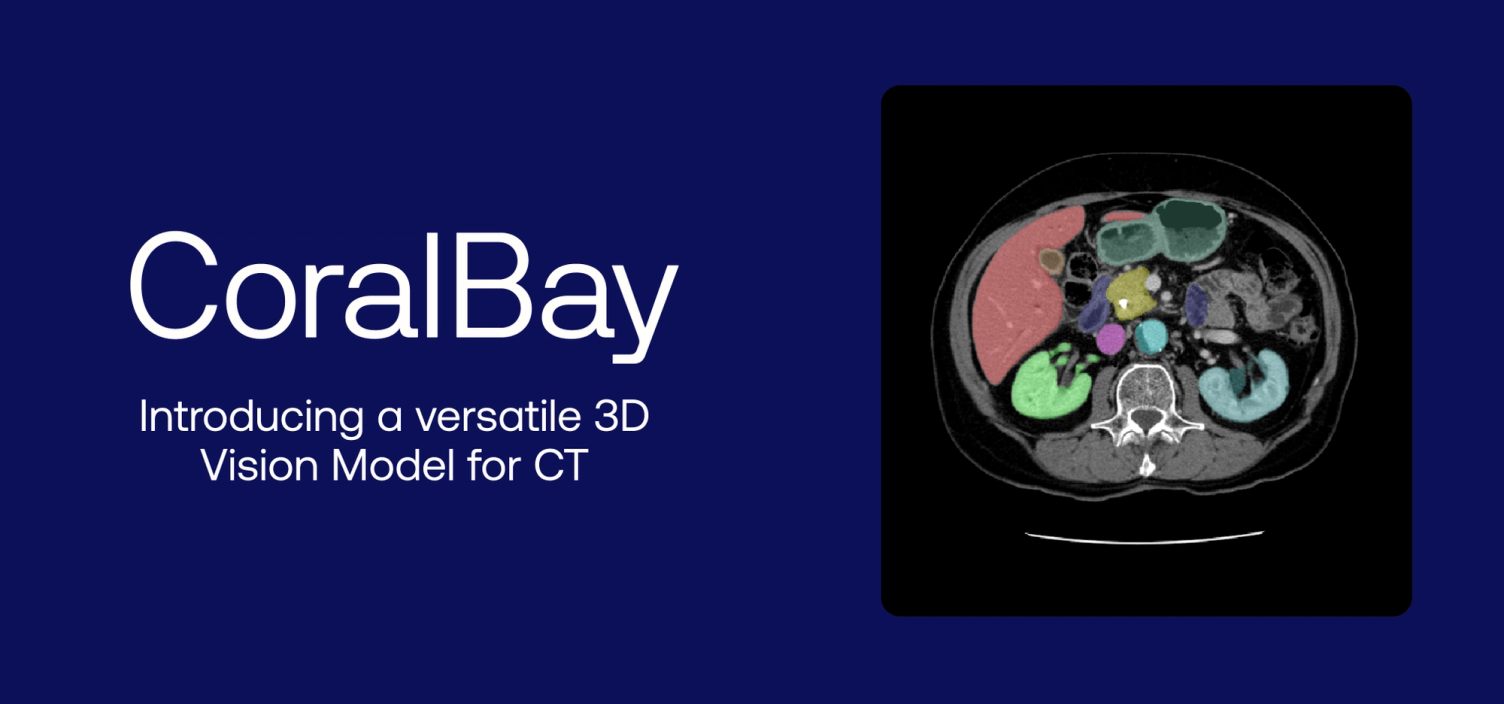
CoralBay
A 3D foundation model for radiology CT, matching far larger models on a fraction of the data. Open-sourced.
Omics and multimodal
Foundation models for genomics and spatial transcriptomics, fusing molecular data with imaging.
Midnight
State-of-the-art pathology foundation models trained on orders of magnitude fewer slides. Open-sourced.
Pathology foundation models
Our first foundation model, trained from public data to hospital scale, with eva, our open framework for evaluating them.